Education in Conflict Situations
Education in Conflict Situations
Date | 12 August 2025
Tomorrow (13 August), the African Union (AU) Peace and Security Council (PSC) will convene its 1296th open session, focusing on education in conflict situations.
The Permanent Representative of Algeria to the AU and Chairperson of the PSC for the month of August 2025, Mohamed Khaled, will deliver opening remarks, followed by Bankole Adeoye, AU Commissioner for Political Affairs, Peace and Security (PAPS). The PSC will receive presentations from Prof. Mohammed Belhocine, Acting Commissioner for Education, Science, Technology and Innovation (ESTI) and Wilson Almeida Adao, the Chairperson of the African Committee of Experts on the Rights and Welfare of the Child (ACERWC). Rebecca Amuge Otengo, Permanent Representative of Uganda to the AU, and Co-Chair of the Africa Platform on Children Affected by Armed Conflicts (AP-CAAC) and the Representative of the United Nations Children’s Fund (UNICEF), will also brief the session.
The last time the PSC convened a session on the theme was at its 1229th meeting, held in August 2024. In that session, the PSC resolved to institutionalise education in conflict as an annual thematic focus. It also stressed the need to uphold the right to education for all, even in conflict, urging Member States to adopt conflict-sensitive, crisis-resilient policies, strengthen data-driven policymaking, integrate inclusive education into post-conflict recovery and appoint a Special Envoy on Children in Conflict. The upcoming session also precedes the 2025 AU Education Summit, intended to mobilise Member States and stakeholders around the continent’s educational priorities. The session is expected to first examine the current state of education in conflict and post-conflict settings, with attention to the systemic collapse of educational services caused by ongoing violence and institutional fragility.
Armed conflict and instability are significant barriers to education in Africa, depriving millions, especially girls, children with disabilities and displaced populations, of safe and inclusive learning. Attacks on schools, the militarisation of facilities and child recruitment erode national education systems, deepening poverty and inequality. In many conflict zones, school closures remove vital protection and create a causal link between attacks on education and the rise in harmful coping mechanisms, particularly child marriage. The loss of schooling exposes adolescents, especially girls, to heightened risks of violence, displacement and economic hardship, reinforcing cycles of vulnerability and deprivation.
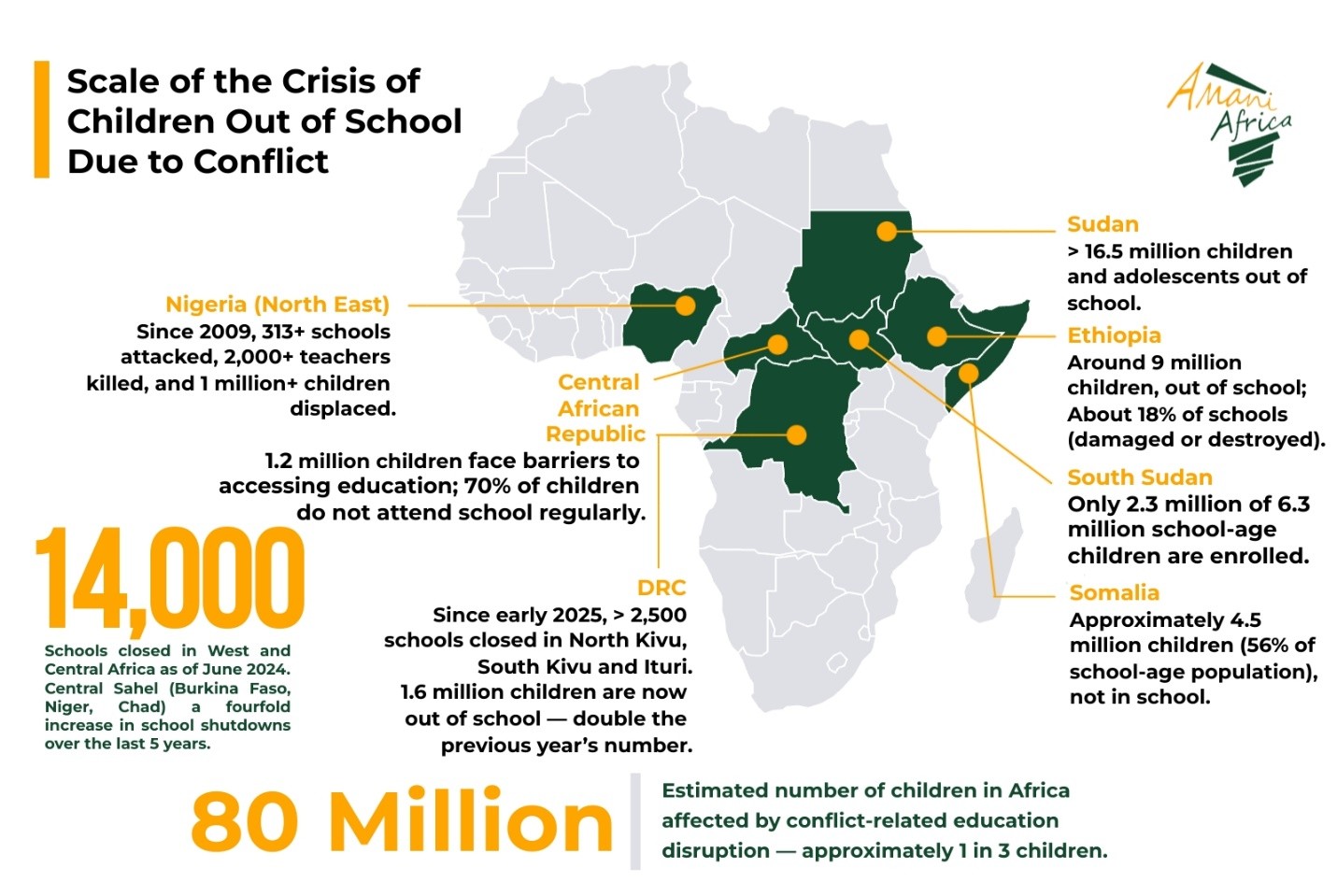
Conflict continues to severely undermine access to education across Africa, with an estimated 80 million children affected, amounting to ‘one in three’ on the continent. In West and Central Africa, insecurity has led to the closure of over 14,000 schools as of June 2024. The Central Sahel region has seen a ‘fourfold increase’ in school shutdowns over the past five years, disrupting education in Burkina Faso, Niger and Chad.
The gravity of the situation is most acute in Sudan, where the ongoing armed conflict has produced one of the continent’s worst education emergencies. Recent estimates place the number of out-of-school children and adolescents at over 16.5 million. Many of these children reside in displacement sites, often with no access to formal education. Prolonged violence has severely disrupted learning, with attacks on schools and the militarisation of educational facilities compounding an already fragile system.
In Ethiopia, an estimated 9 million children remain out of school due to the compounded impact of conflict, climate-related disasters and displacement. Around 18% of educational institutions have either been damaged or destroyed, particularly in conflict-affected regions. This has further aggravated school dropout rates and negatively affected female students, especially in rural and border areas.
In Somalia, data from humanitarian partners indicate that approximately 4.5 million children—representing 56 per cent of the school-age population—are currently out of school. Insecurity, displacement and a lack of access to basic services have left children particularly vulnerable to violence, exploitation and recruitment by armed groups.
In the Central African Republic, conflict continues to affect education severely. Despite a reduction in violence in some areas, 1.2 million children still face significant barriers to schooling, with ‘seven out of ten’ not attending classes regularly. The country has also witnessed attacks on education infrastructure, further straining the capacity of national authorities and humanitarian partners to deliver education in affected areas.
In Nigeria, the northeast region has suffered for over a decade of insurgency. Since 2009, more than 313 schools have been attacked, over 2,000 teachers have been killed, and more than one million children have been displaced. Boko Haram’s systematic targeting of education represents one of the clearest cases of education being weaponised as part of a broader ideological conflict.
In South Sudan, protracted violence has left ‘only about 2.3 million of the country’s 6.3 million school-age children’ enrolled in school. Conflict-related displacement, combined with inadequate infrastructure and limited teacher deployment, continues to hinder educational progress, especially for children residing in camps or border regions.
In the Democratic Republic of Congo (DRC), more than 2,500 schools in the eastern provinces of North Kivu, South Kivu and Ituri have been closed since early 2025. Many of these buildings have been damaged or repurposed, leaving an estimated 1.6 million children out of school in the region—nearly double the previous year’s figures.
In this context, the open session is expected to consider a broad range of strategic responses, including urging Member States to accelerate the domestication and effective implementation of the Safe Schools Declaration (SSD), adopted in 2015 and endorsed by 33 African states. This global intergovernmental commitment seeks to advance the protection of education, restrict the use of schools and universities for military purposes, collect data on attacks against educational facilities and victims, ensure the continuation of learning during conflict and investigate violations to deliver justice and assistance to survivors. These efforts form part of a broader agenda to prevent the military use of educational facilities, strengthen legal protections for learners and educators and establish local monitoring and reporting mechanisms for attacks on education. Within this framework, discussions are anticipated to align with the Continental Education Strategy for Africa (CESA) 2026–2035, particularly Strategic Area 6, which prioritises inclusive education for marginalised and crisis-affected populations.
A key priority will be ensuring the continuity of learning during emergencies. Integrating education contingency planning into national crisis response strategies is expected to be one of the discussion points in tomorrow’s session, reflecting commitments articulated in the Nouakchott Declaration of December 2024 that declares 2025-2034 as the ‘AU Decade of Accelerated Action for Education Transformation, Youth Skills Development and Innovation in Africa’. The declaration commits to safeguarding the right of children and youth to quality education in all circumstances, including during conflict; integrating education in emergencies into national education strategies to enhance system resilience; ensuring schools are protected from attack or military use in line with the SSD; advancing peace education and safe learning environments by embedding violence prevention and response in curricula and adopting conflict-sensitive approaches, especially in humanitarian and fragile contexts; and promoting peaceful conflict resolution while supporting the AU’s ‘Silencing the Guns by 2030’ initiative to foster inclusive learning, particularly in protracted crises. The PSC is expected to promote contingency planning, mobile classrooms and alternative forms of delivery such as digital and radio-based learning—backed by the AU Digital Education Strategy (2023–2028). Enhanced capacity-building for local education actors, support for trauma-informed education and better coordination with civil society are likely to be encouraged to sustain educational continuity in crisis-affected regions.
The session is also expected to devote substantial attention to the psychosocial impacts of conflict on learners. The recent 1290th meeting voiced concern over the rising recruitment of children by armed forces and groups, noting that released children often face severe psychological distress, social stigma and exclusion from education. In response, the current session is likely to advocate integrating mental health services into education systems and providing trauma-informed teacher training to build resilience, improve learning outcomes and prevent long-term harm. Echoing the 597th meeting’s alarm over sexual violence and attacks on educational infrastructure, the PSC may revisit calls—aligned with UN Security Council Resolutions 2143 (2014) and 2225 (2015)—to deter the military use of schools.
Discussions may also explore the link between conflict and the high prevalence of out-of-school children, including those recruited as child soldiers, as highlighted in the 706th meeting’s call for robust child protection frameworks within the AU Commission covering education, health and security. Emphasis may be placed on AU instruments such as the African Charter on the Rights and Welfare of the Child, particularly Article 22, prohibiting child recruitment, and on ensuring the protection and care of children who are affected by armed conflicts. The PSC could further call for stronger coordination between the AU’s Departments of Social Affairs and PAPS to address these issues comprehensively. Stronger inter-ministerial frameworks and improved cooperation between AU bodies such as the African Humanitarian Agency and African Risk Capacity could be highlighted as critical to delivering holistic and effective responses.
Furthermore, education in peace support operations (PSOs) will be addressed as a pillar of post-conflict reconstruction and development (PCRD). Embedding peace education, supporting the reintegration of former child soldiers through education and training peacekeepers to protect learning spaces will all be positioned as strategic components of broader peacebuilding agendas.
Particularly significant for the session is the expected focus on the critical challenge of financing education in emergency settings. Among the proposals likely to be explored are the establishment of pooled funding arrangements and the targeted use of the AU Peace Fund to finance infrastructure rehabilitation, teacher deployment and trauma-informed educational programming. Mobilising adequate and sustained financing, notably to support education for children affected by conflict, will require stronger coordination and alignment of donor contributions with continental frameworks.
The other important area of deliberation is expected to be strengthening data and monitoring systems. Improving the AU Education Management Information Systems (EMIS) could be explored as a strategy to enhance policies and practices that reinforce Member States’ national education systems, to achieve equitable quality education for all (Sustainable Development Goal (SDG 4)) and accelerating CESA implementation. This may include promoting EMIS use to track attendance, safety and learning outcomes in conflict settings, as well as supporting Member States in reporting on SDG 4.
The expected outcome of the session is a communiqué. The PSC may voice grave concern over armed conflict’s impact on education and its implications for Agenda 2063, reaffirming Member States’ commitment to safeguarding education in conflict and post-conflict contexts. It may urge integration of protection and recovery measures into AU PSOs and PCRD frameworks with accountability mechanisms, call for stronger coordination across sectors, increased domestic funding, and alignment of international support with CESA 2026–2035 and Agenda 2063. The PSC could recommend AU Guidelines on Education in Conflict, commission a Health, Humanitarian Affairs and Social Development (HHS)–ESTI study on links between attacks on education and harmful practices, and push for faster domestication and implementation of the SSD. It may also promote integrating child protection and education into the Silencing the Guns initiative, encourage endorsement of the SSD by non-signatories and strengthen implementation by signatories. It may also emphasise stronger coordination among AU sectors working on education, peace and security, humanitarian affairs and social development, and propose a continental platform or task force to monitor and respond to education crises in line with the CESA Cluster on Education in Emergencies. Additionally, it could propose a continental platform for crisis response coordination and an observatory to track child marriage trends in conflict settings for targeted interventions.
PSC to undertake a field mission to South Sudan as it warns of ‘the potential of a full-scale war’
PSC to undertake a field mission to South Sudan as it warns of ‘the potential of a full-scale war’
Date | 8 August 2025
From 10 to 12 August 2025, the premier standing decision-making body of the African Union (AU), the Peace and Security Council, is scheduled to undertake a preventive field mission to South Sudan. This field visit comes against the background of various and high-level engagements by the AU, including through the PSC, as part of the effort to contain the situation in South Sudan and sustain the transitional process.
Following the eruption of fighting in March this year and the ensuing political and constitutional crisis in South Sudan, concerns have been rising about the risk of the situation unravelling the Revitalised Agreement on the Resolution of the Conflict in South Sudan (R-ARCSS) and precipitating the relapse of South Sudan back to conflict. Since then, the PSC has had three engagements on the situation in Sudan, two of them in the course of March 2025, indicating heightened attention and effort to stabilise the situation and avoid further deterioration.
The most recent engagement of the PSC was when it convened its 1283rd session to receive an updated briefing on the situation in South Sudan on 12 June.
The PSC went further from its earlier pronouncements on the situation in South Sudan in its assessment of the gravity of the situation in the country. Expressing ‘deep concern’ over the deteriorating political and security situation, in the communiqué it adopted, the Council warned about ‘the potential of a full-scale war, in violation of the Ceasefire Agreement, thus reversing all the gains registered thus far… in the implementation of the R-ARCSS.’ The PSC called for an ‘immediate cessation of hostilities’ between the South Sudan Peoples’ Defence Forces (SSPDF), Sudan People’s Liberation Movement-in-Opposition (SPLM/A-IO), the White Army, and all other affiliated groups.’ It reiterated that the R-ARCSS remains the only viable framework for achieving sustainable peace in South Sudan. As it calls on the parties to ‘agree to mediation and pursue genuine dialogue’, the PSC expressed ‘deep concern over the continued detention of Riek Machar Teny, First Vice President of the Republic of South Sudan’ and ‘the dismissal and detention of SPLM-IO officials from the Revitalised National Government of Unity (R-TGoNU), in blatant violation of the R-ARCSS.’ It thus reiterated its call ‘for their immediate and unconditional release and reinstatement.’ The PSC considered these measures to be necessary not only ‘to de-escalate the ongoing political tension’ but also ‘to prevent the total collapse of the R-ARCSS.’
Cognisant of how the erosion of trust and the ensuing breakdown of relations between the leaders of the signatories of the R-ARCSS, the Council urged ‘the pursuit of dialogue aimed at restoring mutual trust and confidence.’ Reaffirming the R-ARCSS as the only viable framework for lasting peace in South Sudan and calling for the signatory parties to use peaceful and legal means to resolve their differences and refrain from undermining the agreement and the coalition under RTGoNU, PSC urged them to respect the provisions of the R-ARCSS and desist from undermining peace.
While the PSC was right in calling for an investigation of all violations of the R-ARCSS and warning that peace spoilers will be held accountable, it did not outline the modalities of how these steps need to be followed up. However, in terms of further steps for addressing the deteriorating situation, the PSC envisaged the deployment of sustained diplomatic efforts. First, it encouraged ‘the Panel of the Wise to continue its engagement and mediation efforts with all actors, and the parties to the R-ARCSS.’ Second, it also encouraged the AU Commission Chairperson ‘to sustain engagements with President Salva Kiir and regional leaders to foster inclusive dialogue, facilitate the release of political detainees and support the full implementation of’ R-ARCSS.’
The PSC’s call on the AU Commission Chairperson to sustain engagement with ‘regional leaders’ is particularly notable considering the influence that Uganda, in particular, has in South Sudan, including as a major guarantor of the R-ARCSS. Indeed, it would be difficult for any mediation effort for de-escalating tension and restoring full commitment of the parties to the R-ARCSS to be effective without harnessing and relying on Kampala’s support and leverage.
The threat that the recent fighting and continuing risk of violence pose to the protection of civilians also received the attention of the PSC. Condemning ‘violence against civilians, particularly women and children,’ which, in its view, constitutes violations of international humanitarian and human rights law, the PSC called for ‘an immediate end to indiscriminate attacks against civilians and civilian infrastructure.’ It also urged South Sudanese authorities to investigate and hold perpetrators accountable ‘while taking immediate action to ensure protection of civilians.’
The other issue that was the centre of discussion during the session, as it had been in recent years, was the implementation of the R-ARCSS. In this respect, apart from encouraging the parties to the Tumaini Initiative and those yet to join ‘to reach a timely consensus for an inclusive peace process,’ the PSC first called on ‘the RTGoNU to expediate the deployment of the Necessary United Forces…facilitate the civic and political space for inclusive engagement.’ Second, it encouraged ‘the South Sudanese parties to commit to implementing all outstanding transitional tasks, such as security sector reform, including undertaking the second phase of the unification of forces, and the harmonisation of the command structure with a national character under one commander in chief.’ This is profoundly critical as success in reform of the security sector and its governance is central to ensuring the fragmentation of the security landscape in South Sudan. Third, it urged the RTGoNU to mobilise resources for the three institutions critical to the implementation of transitional tasks, critical to the holding of elections: the National Elections Commission (NEC), the National Constitutional Review Commission (NCRC) and the Political Parties Council (PPC).
In terms of advancing mediation efforts, the PSC also encouraged the Trilateral Mechanism to work with the RTGoNU ‘to reactivate the Government-Trilateral Joint Task Force (JTF) and facilitate the implementation of pending R-ARCSS provisions, including constitution making and electoral processes.’
The PSC field mission session came following high-level visits to South Sudan, a) by the Panel of the Wise, which the PSC had called for during its 1265th and 1270th sessions, and b) by the Chairperson of the AU Commission and the Deputy Executive Secretary of the Intergovernmental Authority on Development (IGAD). It is expected that the PSC visit will build on these previous engagements of the relevant AU structures, including at the highest levels by the Chairperson of the AU Commission. The visit also affords the PSC an opportunity to follow up on its various previous decisions, as highlighted above from its 1283rd session. Whether the mission succeeds in securing critical concessions and gets the parties back on track for implementing the transitional process will be a major test of whether South Sudan can conclude the transitional process for holding national elections in 2026 and avoid relapse.
This article builds on an analysis of the June 2025 PSC session on South Sudan that first appeared on The Monthly Digest on the PSC for June 2025.
Consultation of PSC with the AGA-APSA Platform/Human Rights Subcommittee
Consultation of PSC with the AGA-APSA Platform/Human Rights Subcommittee
Date | 7 August 2025
Tomorrow (8 August), the African Union (AU) Peace and Security Council (PSC) will convene its 1295th Session for the consultation between the African Governance Architecture-African Peace and Security Architecture (AGA-APSA) Platform and the PRC Sub-Committee on Human Rights, Democracy and Governance (HRDG).
The session is expected to start with an opening statement by Mohamed Khaled, Permanent Representative of Algeria to the AU and Chairperson of the Peace and Security Council of the AU for August 2025 and the introductory remarks by H.E. Ambassador Bankole Adeoye, AU Commissioner for Political Affairs, Peace and Security. Presentations are also expected from Ambassador Willy Nyamitwe, Permanent Representative of the Republic of Burundi, and the Ag. Chairperson of the PRC Sub Committee on Human Rights, Democracy and Governance (HRDG) and Wilson Almeida Adao, Chairperson of the African Committee of Experts on Rights and Welfare of the Child (ACERWC) and Chairperson of the AGA Platform.
The PSC last convened such a consultation during its 1167th session in August 2023, marking the first time it brought together both the AGA-APSA Platform and the PRC Sub-Committee on HRDG in a joint session. Previously, the PSC had engaged with these two bodies separately, holding its inaugural consultation with the AGA-APSA Platform at its 1098th session in August 2022, and a separate meeting with the PRC Sub-Committee during its 1095th session in the same month. Both sessions underscored the importance of these engagements and recommended that joint consultations be held annually. This collaborative approach is not only supported by previous PSC decisions but is also grounded in the PSC Protocol, which mandates the Council to promote democratic governance, the rule of law, and the protection of human rights across the continent. The joint consultation seeks to deepen coordination among PSC Members, the PRC Sub-Committee on HRDG, and the AGA-APSA Platform, fostering a more coherent and impactful response to governance-related peace and security challenges in Africa.

The consultation is expected to deliberate on the engagement of the PRC sub-committee on pressing governance and human rights issues related to peace and security challenges in tomorrow’s session. This is expected to put the spotlight on governance challenges faced on the continent. Beyond the unconstitutional changes of government, the challenges identified include a lack of transparency and accountability, weak institutions, corruption, repression of expressions of dissent, a lack of inclusivity, and increasing disaffection of the majority youthful population with failure of governments to deliver services, as well as human rights violations. Exacerbated by the spread of jihadist violence and growing public disillusionment with civilian leadership, as well as the extension of term limits, inconsistent responses of AGA Platform institutions, including the PSC, have exacerbated the situation. A case in point is the lack of enforcement of Article 25(4) of ACDEG that bars perpetrators of unconstitutional changes of government from participating in elections in two recent cases of Chad and Gabon. This trend undermines the AU’s democratic norms, making it critical for the consultations to meaningfully address the root causes of instability and safeguard the continent’s hard-won peace, security, and democratic governance gains.
The consultation is also expected to focus on the widespread and interconnected conflicts across the continent, with Sudan, the Democratic Republic of the Congo (DRC), South Sudan, and the Sahel serving as key examples of protracted regional conflict systems that are increasingly affected by external meddling, geopolitical rivalry, and the scramble for natural resources. This affords the PRC Sub-committee and the PSC to interrogate the ways in which the changing global geopolitical context is increasingly exacerbating governance challenges and conflict dynamics on the continent and how the AU can leverage AU instruments for mitigating these trends. Discussions will likely examine the persistent challenges in effectively implementing post-conflict reconstruction and development (PCRD) strategies in countries emerging from violence. The session is also anticipated to address recurrent election-related violence, emphasising the urgent need for stronger preventive and governance measures.
Beyond the foregoing, the discussions are expected to also focus on prioritizing the design of joint, coordinated initiatives by leveraging the PSC’s authority, utilizing the AGA platform coordination role, and engaging the PRC Sub-Committee on HRDG oversight function to directly address the root causes of instability, namely, weak democratic institutions, lack of accountability, and governance-related grievances. These initiatives are vital not only for reinforcing AU norms such as the ACDEG but also for enhancing early warning systems, bolstering preventive diplomacy, and grounding post-conflict recovery efforts in democratic consolidation and the rule of law.

Among the key decisions adopted by the PSC in its previous session was a call for a joint consultative meeting between the AU Commission, the African Governance Platform (AGP), and the AGA-APSA Secretariat to identify concrete, action-oriented initiatives that go beyond periodic experience-sharing. These included conducting joint promotional visits by the PSC, the PRC Sub-Committee, and the AGP to advocate for the ratification and implementation of AU shared values instruments. However, no such joint promotional visits have taken place to date. Another component of the decision emphasised the need to involve the PSC in the planning and implementation of AGA Flagship Initiatives and to establish robust follow-up mechanisms to ensure that decisions from joint sessions lead to tangible outcomes. While the PSC has held separate consultations with some AU organs that are members of the AGA-APSA Platform, such as the African Commission on Human and Peoples’ Rights (ACHPR), African Union Economic Social and Cultural Council (ECOSOCC), and African Peer Review Mechanism (APRM), there is currently no clear framework or evidence to assess the extent of the PSC’s involvement in AGA Flagship Initiatives.
In line with the previous decision, tomorrow’s session is expected to prioritise the development of coordinated action plans that facilitate the joint implementation of shared mandates and strengthen synergy between the AU’s governance and peace and security pillars. In this regard, a key development expected to inform the discussions is the ongoing formulation of the Joint AGA-APSA Roadmap. This strategic document aims to serve as a guiding framework for enhancing operational synergy between the governance and peace and security pillars of the AU. Its development responds directly to the PSC’s repeated calls for more structured, outcome-driven engagement between the two architectures. It seeks to move beyond ad hoc collaboration towards a more institutionalised and programmatic partnership. Once finalised, the Joint Roadmap is expected to provide a common results framework that will facilitate alignment of interventions, monitor implementation of joint decisions, and promote a proactive, preventive approach to addressing the root causes of conflict on the continent.
The outcome of the session is expected to be a Communiqué. The PSC is expected to reaffirm its commitment to holding annual joint consultations with the AGA-APSA Platform and the PRC Sub-Committee on Human Rights, Democracy and Governance (HRDG). The Council may also underscore the importance of institutional synergy between governance and peace and security actors in addressing structural drivers of conflict. Concerning governance-related root causes of instability, the PSC may commend ongoing joint efforts to tackle democratic deficits and call for the more consistent application of AU norms, particularly those relating to unconstitutional changes of government, to strengthen their deterrent effect. Regarding the Joint AGA-APSA Roadmap, the PSC is expected to encourage its timely finalisation and adoption as a guiding framework for coordinated action. In the same vein, the Council may reiterate its previous request for the AU Commission to expedite the operationalisation of the African Governance Facility, emphasising its importance for supporting Member States and AGA activities, especially in preventive governance. The PSC may also restate its earlier decision to conduct joint promotional visits, together with the AGP and the PRC Sub-Committee, to advocate for the ratification and implementation of AU shared values instruments. In an effort to enhance the PSC’s role in AGA Flagship Initiatives, the Council is likely to stress the need to develop a precise mechanism for its involvement in the planning, implementation, and monitoring of these initiatives. It may also call for the establishment of a regular reporting channel or periodic briefing mechanism to keep the PSC updated on progress. Furthermore, the PSC may emphasise the need to strengthen collaboration between governance and peace and security actors in early warning and preventive diplomacy, including the conduct of joint assessments and missions to countries facing elevated risks of instability. Similarly, it may highlight the importance of integrating governance dimensions into post-conflict reconstruction and development (PCRD) processes, recommending that governance assessments be considered when mandating AU support to countries emerging from conflict. Lastly, the PSC may request the establishment of a joint follow-up mechanism or working group to monitor the implementation of decisions emanating from this and previous joint consultations, and to report periodically to both the PSC and the PRC Sub-Committee on HRDG.
Assessment of the role of ad hoc governance, peace and security mechanisms in supporting the PSC’s mandate
Assessment of the role of ad hoc governance, peace and security mechanisms in supporting the PSC’s mandate
Date | 5 August 2025
Tomorrow (6 August), the African Union (AU) Peace and Security Council (PSC) will convene its 1294th session to assess the role of ad hoc governance, peace, and security mechanisms in supporting the PSC’s mandate.
The session will commence with opening remarks by Mohamed Khaled, Permanent Representative of Algeria to the AU and Chairperson of the PSC for August 2025, followed by introductory remarks from Bankole Adeoye, AU Commissioner for Political Affairs, Peace and Security (PAPS). Solomon Dersso, Founding Director of Amani Africa Media and Research Services, will also deliver a presentation.
Following the establishment of the PSC and the structures for the implementation of its conflict prevention, management and resolution decisions, the AU has been enterprising in the tools/instruments that it has innovatively designed and implemented for peacemaking and mediation. The most notable of these innovations was the use of ad hoc governance and peace and security mechanisms instituted in support of the mandate of the PSC. As elaborated in The African Union Peace and Security Council Handbook: Guide on the Council’s Procedure, Practice and Traditions, the use of these mechanisms is built on the provisions of the PSC Protocol.
Article 6(c) of the Protocol Relating to the Establishment of the Peace and Security Council of the African Union PSC mandates the Council to engage in ‘peacemaking, including the use of good offices, mediation, conciliation, and enquiry’. To effectively implement these mandates, the Protocol further authorises the PSC to establish subsidiary bodies as needed. In particular, Article 8(5) provides that the PSC may create such bodies, including ad hoc committees, as it deems necessary to undertake specific tasks such as mediation, conciliation, or fact-finding enquiries.
These high-level peacemaking and mediation tools that the AU instituted as instruments for the management and resolution of crisis and conflict consist, mainly, not exclusively, of:
- ad hoc committees for mediation consisting of leaders of a group of states (Art. 8(5) of the PSC Protocol) and
- High-level panels.
These ad hoc governance, peace and security mechanisms are often established by the PSC under the authority vested in it by its Protocol, but they are also at times instituted by the AU’s supreme authority, the AU Assembly.
While Article 8(5) of the PSC Protocol envisages the use of ad hoc committees, it did not spell out the level at which such a committee would be established and the form such a committee would take. One of the innovations of the PSC was to constitute the ad hoc committee as an instrument of peacemaking from sitting heads of state and government. For the first time, the PSC established an ad hoc committee at the level of heads of state and government in respect to the conflict in Côte d’Ivoire in January 2011. It was during its 259th session that the PSC decided to establish such a committee, called at the time a high-level panel, for the resolution of the (post-election) crisis in Côte d’Ivoire. The committee was made up of President Mohammed Ould Abdel Aziz of Mauritania, President Jacob Zuma of South Africa, Blaise Campaore of Burkina Faso, Jakaya Kikwete of Tanzania and Idriss Deby Itno of Chad. Since then, the PSC and the AU Assembly have established ad hoc committees in relation to conflict situations in Libya, South Sudan, the AU Summit Troika on Western Sahara and Sudan.
The make-up of these ad hoc committees, from representatives of the five regions of the continent, sought both to ensure ownership of the peace process by all parts of the continent and to enlist the support and engagement of the wider membership of the AU. The fact that the body is also made up of leaders of AU member states that are not necessarily members of the PSC helps create separation of powers for healthy checks and balances. The fact that the ad hoc committees relied on sitting Heads of State and Government also signifies that the situation warrants the attention of the highest authority of AU member states and is indicative of AU’s diplomatic acumen to use the leverage of current leaders from across the continent in the search for a resolution of the situation. As the use of this mechanism for a post-election crisis in Côte d’Ivoire illustrates, these ad hoc committees are deployed not only for peace and security but also for governance crises.
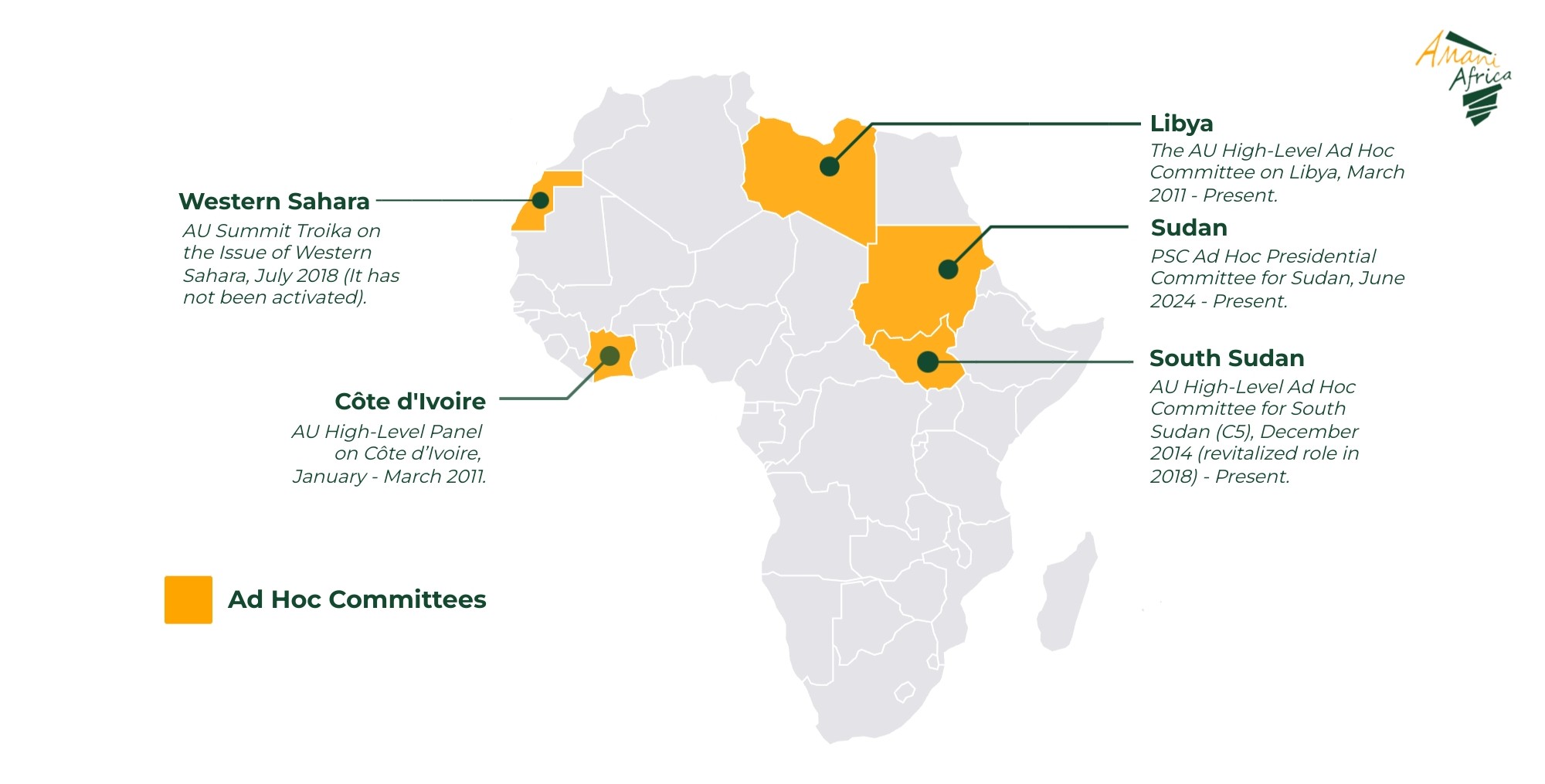
The second group of ad hoc mechanisms for governance, peace, and security deployed by the PSC, which is a complete innovation of the PSC, concerns the high-level panels. The first instance in which the PSC exercised this power was in July 2008, during its 142nd session, when it requested the AU Commission to establish a High-Level Panel on Darfur. Since then, several ad hoc mechanisms have been constituted (see map below for the list of AU ad hoc committees and high-level panels). While most of these mechanisms are initiated by the Council itself, there are also instances where the Chairperson of the AU Commission initiated the mechanisms, with the PSC’s endorsement. The High-Level Panel on Egypt and the mediation process in Ethiopia are examples of such cases. It is, however, worth noting that prior to its use in Sudan, such a high-level panel was constituted by the AU Assembly Chairperson, President John Kufuor of Ghana, in 2008 under the leadership of Kofi Annan for mediating the post-election violence in Kenya.

As the precedent-setting experience of the AU High-level Panel on Darfur and that later transitioned into the AU High-level Implementation Panel on Sudan shows, one of the notable aspects of the peace and security entrepreneurship of the AU in deploying these mechanisms was the use of former heads of state and government. This not only resonates with Africa’s diplomatic and political tradition that cherishes the wisdom of elders but also represents a recognition of the importance of the experience and peer level access that former leaders possess, thereby making them positioned to navigate complex political issues by leveraging their standing and political insights into the dilemmas and concerns that inform the actions of leaders.
It was the effective utilisation of these ad hoc mechanisms during the first decade and a half of the existence of the AU and its PSC that effectively established the role of the AU as the lead peace and security and governance management actor on the continent. Indeed, the experience from these ad hoc governance and peace and security mechanisms offers useful insights into how to re-assert the leadership role of the AU and reposition the African Peace and Security Architecture for a changing global and continental governance and peace and security context. This is particularly critical considering the prevailing context that characterises the time when tomorrow’s session is taking place. One of the features of this period is the decline in AU’s peace and security and governance management role. The combination of the slow pace of response of the AU and the lack of robust political support for its peace and security initiatives as well as the emergence of increasingly assertive states vying for individual mediation role means that increasingly the space for peace and security initiative on African situations such as the Democratic Republic of Congo (DRC)-Rwanda and Ethiopia-Somalia tensions and the conflict in Sudan is being taken by non-African states such as Qatar/US, Turkey and Saudi Arabia/US.
In this regard, tomorrow’s session offers a timely opportunity for introspection—to reflect on past and current mediation experiences, particularly those involving ad hoc committees and high-level panels, and their role in advancing PSC’s mandate. What key insights and lessons can the PSC draw from these experiences? The session also takes place against the backdrop of ongoing efforts to review the African Peace and Security Architecture (APSA), including the establishment of a high-level panel by the AU Champion for Institutional Reform, President William Ruto of Kenya. This reflection, therefore, could provide valuable input into the review process.
The analysis of the experience of the ad hoc mechanisms shows that while they have formed part of the AU’s innovative major governance crises and conflict management and resolution tools over the past 15 years, their success has varied. Notably, the AU High-Level Panel on Darfur (AUPD), chaired by former South African President Thabo Mbeki, delivered a landmark analysis that reframed the conflict in Darfur as a manifestation of a broader crisis of governance in Sudan and provided the AU with a clear roadmap on how best the structural issues of peace, justice, reconciliation and healing could be addressed in Darfur. Building on this, the AU High-Level Implementation Panel (AUHIP) was established to implement the AUPD’s recommendations and subsequently to mediate post-secession negotiations between Sudan and South Sudan. By actively seeking and enlisting the support of the region, the PSC, the UNSC and the Troika of the US, UK and Norway, through a clear definition of the issues based on a deductive approach and anchored on a highly professional and technically endowed supporting structure as well as exemplary diplomatic leadership willing and able to dedicate sustained engagement and attention, the AUHIP set the template for successful mediation that registered notable successes including midwifing the peaceful secession of South Sudan and the building of a relatively peaceful post-secession outcome between Sudan and South Sudan. The AUHIP, leveraging the PSC and the UNSC, played a decisive role in averting full-scale war between the two countries following the Heglig crisis in April 2012 and, with the support of IGAD and Ethiopia, brokered eight historic Cooperation Agreements in September 2012 addressing critical post-secession issues. Widely hailed as a ‘wide-ranging, detailed, and historic set of treaties,’ these agreements covered nearly every key aspect of Sudan–South Sudan relations. Equally, if not more successful, experience was the Kofi Annan-led Panel of Eminent Persons that mediated the post-election violence in Kenya.
Meanwhile, other ad hoc mechanisms, such as the PSC ad hoc Presidential Committee for Sudan, have as yet made no headway. Despite being established over a year ago, the ad hoc Presidential Committee has yet to convene its inaugural meeting, even as the conflict escalates and the country edges closer to de facto fragmentation. While the high-level committee on Libya did not succeed in its effort to avert Libya’s descent into state fragmentation and violent conflict, the High-Level Ad Hoc Committee’ (C5) on South Sudan was one of the catalysts for breaking deadlocks between the parties to the Revitalised Agreement for the Resolution of the Conflict in South Sudan (R-ARCSS) that threatened at various points the transitional process in South Sudan.
The analysis of the various ad hoc committees reveals that there are certain factors that are critical for successful AU-led peacemaking and mediation diplomacy. The first of these concerns the composition of the members of the mechanisms and the quality of leadership of the mechanisms. The composition of the mechanism should involve those who not only hold high-level positions—such as former or current heads of state or government—to provide the necessary political and diplomatic weight but also have the tenacity and temperament for providing the process befitting the nature of the crisis or conflict situation. The second lesson is the need for a solid mediation strategy and process that ensures sustained engagement, as illustrated by the AUHIP as opposed to the improvisation-heavy and touch-and-go approach that seems to be the current characteristic of the AU High-level Panel on Sudan. The third lesson highlighted in the Lessons Learned Report from the AU-Led Peace Process for the Tigray Region, Ethiopia, is the need for appointing personalities that have the full confidence of the parties. With Olusegun Obasanjo, who was appointed in August 2021 as the High-Representative of the AU Commission Chairperson charged with facilitating the resolution of the conflict in Tigray, facing charged of bias by one of the parties, it was the decision by the AU to appoint a panel of mediators with the addition of two additional mediators that created the balance that won the full confidence of the parties who agreed to be convened under its facilitation. The other lesson for the success of ad hoc mechanisms from AUHIP to the Ad hoc Committee of 5 on South Sudan to the AU High-Level Panel on the Ethiopian Peace Process is the imperative for strong coordination with and mobilisation of support from key regional and international actors. Not any less significant is the quality of the support structure, including qualified technical experts and adequate financial resources, that is put in place for facilitating the effective functioning of the ad hoc mechanism. The African Union Panel on Darfur (AUPD) benefited from the contributions of nine prominent experts, while the African Union High-Level Implementation Panel (AUHIP) drew on a wide range of technical expertise from across the globe, including specialists in oil, economics, law, border demarcation, and other relevant areas. This expert input was further complemented by support from AU staff. AUHIP is not unique in this. The panel of mediators led by Kofi Annan that was enlisted to mediate the post-election violence in Kenya in 2008 by the then Chairperson of the AU Assembly, Ghana’s President John Kufuor, similarly enjoyed a robust support structure. Some of the current mechanisms, such as the AU High-level Panel on Sudan, do not seem to be as endowed with such robust structures as the AUHIP or the Kofi Annan-led AU mediation on the post-election crisis in Kenya. In terms of mobilisation of requisite financial support, the AU’s partnership with the African Development Bank (AfDB), which availed funding for the Ethiopia mediation process, offers a useful example of leveraging the contribution of various entities in supporting AU ad hoc mechanisms.
The expected outcome is a communiqué. The PSC is expected to underscore the vital role of ad hoc governance, peace, and security mechanisms in fulfilling its mandate on conflict prevention, management, and resolution. It may reaffirm the importance of the ongoing APSA review as a necessary step for the AU to adapt to evolving regional and global dynamics. While welcoming the ongoing efforts in this regard, the PSC may use the opportunity to highlight the need to revitalise the AU’s preventive diplomacy and mediation efforts, and to re-establish diplomacy as the primary instrument for achieving peace and security on the continent. In this context, the PSC may stress the importance of enhancing the use of ad hoc mechanisms as part of the APSA review process, drawing on insights and lessons learned from successful past experiences in deploying these mechanisms across Africa. Emphasising the need for a robust support system to ensure the effective functioning of these mechanisms, the PSC may also call for the strengthening of the AU’s conflict prevention, management, and resolution structures, particularly the Mediation and Dialogue Division, the Continental Early Warning System and the Panel of the Wise.
Briefing on the situation in Sudan
Briefing on the situation in Sudan
Date | 3 August 2025
Tomorrow (4 August), the African Union (AU) Peace and Security Council (AUPSC) will hold its first session of the month to consider the situation in Sudan.
The session will commence with an opening remark by Mohamed Khaled, Permanent Representative of the People’s Democratic Republic of Algeria to the AU and Chairperson of the Peace and Security Council (PSC) for August 2025. This is followed by introductory statement from Bankole Adeoye, AU Commissioner for Political Affairs, Peace and Security. A representative of the Intergovernmental Authority on Development (IGAD) is also expected to make a statement. It is also envisaged that the PSC receives a statement on the humanitarian situation, including access to humanitarian assistance and food insecurity, from Haneed Nuru, Director of the World Food Programme African Union Global Office. Since Sudan is suspended following the October 2021 coup that laid the foundation for the eruption of the conflict in April 2023, it would not accordingly be invited to make a statement during the session.
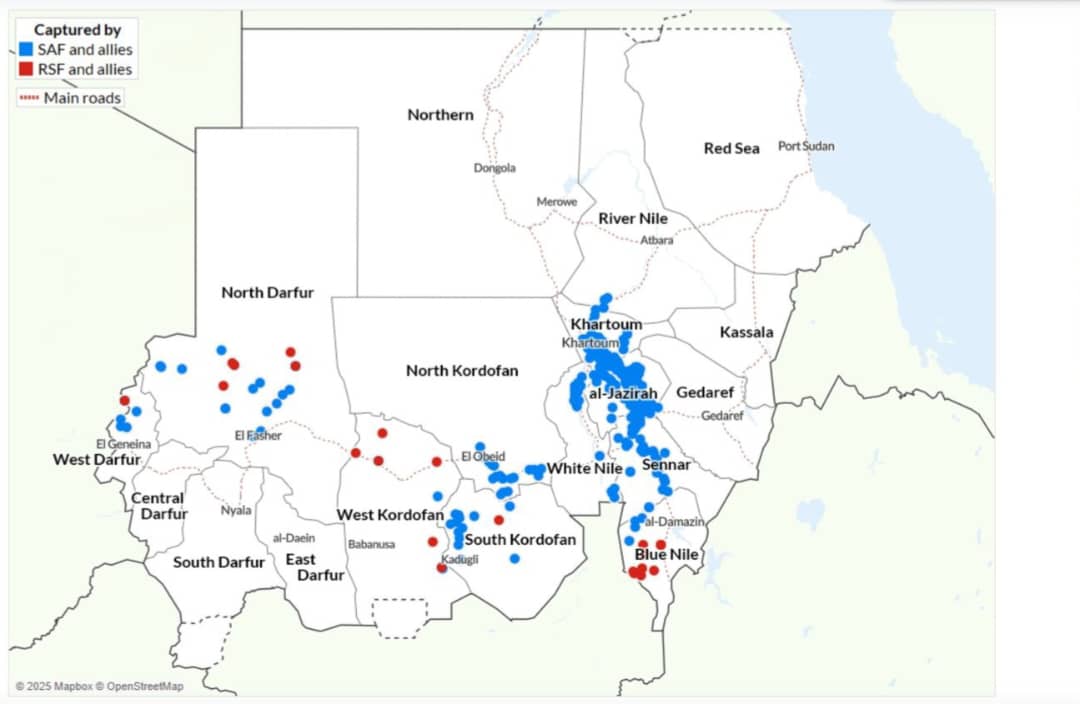
There have been major developments since the PSC’s last substantive session in February 2025. The frontlines of the fighting and the territorial control of the major parties to the war – the Sudan Armed Forces (SAF) and the Rapid Support Forces (RSF) have substantially shifted. At the end of March, the SAF succeeded in wresting control of Khartoum from RSF. On its part, the RSF expanded its offensive in May to the East by launching long-range drone attacks that targeted various cities, including Port Sudan. These attacks targeted key civilian and military infrastructure, including the international airport, a military airbase, fuel depots, and power stations.
Despite shifts in the battlefield dynamics, the warring parties remain entrenched in their positions and appear determined to pursue a military solution. As each tries to consolidate its respective areas of control and inflict loss on the other, the focus of the terrain of fighting has shifted. As a result, the fighting now appears to be shifting southward into Kordofan and eastward in Darfur. The ongoing fighting in Kordofan has reportedly resulted in the massive displacement of people and the collapse of essential services. As the RSF shifted its focus to consolidate its control in Darfur, it intensified its siege and attacks on North Darfur’s capital, El Fasher, through shelling, drone strikes, and ground operations, exacerbating the already dire humanitarian and hunger conditions in the besieged city and its environs. In July, the United Nations called on the warring parties to agree to a humanitarian pause in the besieged city. While the Sudanese Armed Forces (SAF) reportedly accepted the proposal, the Rapid Support Forces (RSF) rejected it. Indicating further expansion of the war front, in June, the RSF claimed control of the tri-border area of Egypt, Libya, and Sudan, both to expand the supply line through Libya and extend the fighting into the Nile Valley and Northern State.
With the war showing no sign of abating, the dire humanitarian situation continues to deteriorate, as the statement from the WFP representative would make clear. Indiscriminate attacks against civilians continue. The RSF long-range drone attacks targeted not only military targets but also civilian infrastructures, including the 10 May 2025 bombing that attacked the central prison in El Obeid, reportedly resulting in the death of 29 prisoners and injuring dozens more. In an incident attributed to the SAF, the bombing on 21 June on the Al-Mujlad hospital in West Kordofan reportedly resulted in the killing of more than 40 people, including six children and five healthcare workers. Sudan remains the world’s largest humanitarian crisis, with over 30 million people in need of assistance.
As they both deepen their effort to consolidate their respective territorial control, they are also seeking to translate territorial control into political influence. SAF has regained control over parts of the east and centre of the country, including the capital, Khartoum. Meanwhile, RSF is working to consolidate its hold in the west and south, particularly in Darfur and South Kordofan. In May, General Abdel Fattah al-Burhan, head of Sudan’s Transitional Sovereignty Council, appointed Kamal Idris as the new prime minister. Idris subsequently dissolved the existing government in June and is currently consulting on the formation of a new cabinet. On 26 July, the RSF-led coalition, known as the Tasis Alliance, also announced the formation of a parallel government, with RSF commander Mohamed Hamdan Dagalo appointing Mohamed Hassan al-Ta’ishi as prime minister.
The emergence of rival governments in the respective territorial spheres of influence of the two rival warring parties has raised renewed fears of Sudan’s potential fragmentation, drawing comparisons to the situation in Libya. It is against this backdrop that tomorrow’s session is scheduled. The UN Security Council is also set to hold closed consultations on the situation in Sudan on the same day.
Tomorrow’s session comes less than a week after the PSC issued a statement. The statement, issued on 29 July, was issued in direct response to and with exclusive focus on the 26 July 2025 announcement by the Rapid Support Forces (RSF) of the establishment of a parallel civilian administration, referred to as the Sudan Founding Alliance (Tasis) in areas under its control. This is not the first time the PSC has issued a statement condemning the RSF’s initiative for establishing a parallel government. Condemning the announcement on the establishment of such a parallel government by the RSF, in an earlier statement issued on 11 March, the PSC warned that ‘such action carries a huge risk of partitioning of the country.’ While both statements explicitly stated that the PSC does not recognise the parallel government, reaffirmed the unity and territorial integrity of Sudan and urged all AU member states and the international community not to recognise any parallel government, the 11 March statement additionally reaffirmed the AU’s ‘unwavering commitment to continue to collaborate with all Sudanese stakeholders towards finding viable and durable solutions towards silencing the guns permanently in Sudan’ on the basis of the AU roadmap (emphasis added). By contrast, in a clear departure from this ‘commitment to continue to collaborate with all Sudanese stakeholders’, the 29 July statement asserted that the ‘African Union only recognises the Transitional Sovereign Council and the recently formed civilian transitional government.’ The ‘civilian transitional government’ that this statement makes reference to is the appointment by Chairman of the Transitional Sovereign Council, General Abdel Fattah Al Burhan, Sudan Armed Forces (SAF) chief, of Kamil al-Tayeb Idris as a civilian Prime Minister. The PSC’s recognition of the so-called ‘civilian transitional government’ follows the statement of 30 May 2025 by the AU Commission Chairperson, who described the appointment of the prime minister ‘as a step towards inclusive governance’.
There are fears that this shift in the policy position of the PSC and the AUC may resuscitate the agenda of lifting the suspension of Sudan from the AU. However, there is no inclusive political process and national dialogue involving diverse political and social forces of Sudan, nor is there any transitional roadmap developed through such a political process and national dialogue. With the war raging on with no end in sight, neither national constitution-making nor general national elections are on the horizon. As the recent experience in Gabon illustrates, even with such processes and a roadmap, the constitutional order is not considered to have been restored before the convening of general national elections. As such, any lifting of the suspension of Sudan at this point could not happen without breaking the AU norm on unconstitutional change of government.
Despite the worsening security and humanitarian situation in the Sudan, ongoing mediation efforts aimed at reaching a diplomatic resolution have made limited progress, with little prospect of securing a ceasefire. The involvement of multiple actors in these initiatives has further complicated the peace process. In May, the United Nations, African Union, and the League of Arab States held a tripartite meeting in Baghdad, Iraq, aimed at promoting greater synergy in their engagement on the Sudan file. They apparently intend to include IGAD in future meetings under this format. In June, the European Union convened a consultative meeting in Brussels on enhancing coordination of peace initiatives and efforts for Sudan, bringing together several key actors involved in the peace process. The next meeting is expected to take place in Addis Ababa.
In the meantime, the United States appears to be shifting its focus to Sudan, building on its recent success in mediating between the Democratic Republic of Congo and Rwanda. It had planned to host a meeting of the Quad—comprising Egypt, Saudi Arabia, and the United Arab Emirates—in Washington, D.C., on 30 July, with the aim of advancing the Sudan peace talks. However, the meeting was reportedly postponed due to disagreements over the anticipated outcome. Similarly, an earlier conference on Sudan convened by the United Kingdom in London in April failed to produce results, also due to disagreements over the terms of a joint declaration.
The ongoing conflict in Sudan has been further complicated by the involvement of external actors and the use of modern warfare technologies, including unmanned aerial vehicles. Despite the existing UN arms embargo, the flow of weapons into the country has continued unabated, fueling the violence and having a devastating impact on civilians. The conflict has also had far-reaching consequences for the broader region.
All seven of Sudan’s neighbouring countries have been affected to varying degrees. In particular, the situation in Abyei—a disputed border area between Sudan and South Sudan—has significantly worsened. The conflict has exacerbated intercommunal tensions, increased displacement, and undermined ongoing peace efforts. The spillover effect has also been evident in the presence of RSF elements across borders and a sharp increase in cross-border movements, including refugees and returnees. Recent fighting in the tri-border area of Sudan, Libya, and Egypt involving SAF, RSF, and armed groups affiliated with the Libyan National Army—led by General Khalifa Haftar—has raised concern that it could spark another regional tension.
The expected outcome of the session is a communiqué. The PSC is expected to express its grave concern over the continuation of fighting in Sudan without any sign of a major breakthrough for peace. It may reiterate its earlier calls on the imperative for ending the fighting in Sudan, calling for a ceasefire and cessation of hostilities. It may also condemn the indiscriminate attacks targeting civilians, including the incidents that led to civilian deaths in El Obeid and West Darfur, and state that those responsible for violations against civilians will be held accountable. The PSC may also call for an end to hostilities in Kordofan and the lifting of the siege that the RSF imposed on El Fasher, worsening the dire humanitarian and hunger crises in the city and its environs. It may also reiterate the imperative for unhindered and safe humanitarian access to ameliorate the humanitarian catastrophe and urge the parties to ensure civilian protection. It is expected that the PSC will restate its position expressed in the 11 March 2025 and 29 July 2025 statements, rejecting and condemning the establishment of parallel governments by the RSF and calling on all AU member states and the international community not to recognise the establishment of the parallel government announced by the RSF on 26 July 2025. While the PSC may not return to its 11 March 2025 statement in which it expressed AU’s commitment to continue to collaborate with all Sudanese stakeholders, it may make it clear that its recognition of the Transitional Sovereign Council in pursuit of safeguarding the territorial integrity of Sudan does not dispense with the need for a political process for the establishment of an all-inclusive transitional government and for finding diplomatic resolution of the current conflict. It may, in this regard, reaffirm its commitment to the May 2023 AU roadmap for the resolution of the conflict in Sudan and that there can be no military solution to the conflict in Sudan. The PSC may also affirm the need for an all-inclusive political process and national dialogue for developing a transitional roadmap, covering constitution-making and holding of general national elections, in order to achieve restoration of constitutional order, for which bringing the war to an end is essential. On the peace process, the PSC is expected to call for the integration of all initiatives for peace in Sudan into a single process. It may also call for the AU to assert a leading role in facilitating such a single peace process for Sudan.
The Imperative for and Outline of a New Paradigm for Africa's International Relations in a Fundamentally Changing Global Order
The Imperative for and Outline of a New Paradigm for Africa's International Relations in a Fundamentally Changing Global Order
Date | 31 July 2025
INTRODUCTION
The global order is going through a historic transformation. There is a profound shift in the structure of the power relations between states. While the state system remains the basis of the global order, the role and power of the state have hugely diminished. Of particular significance is the fact that the old order is in the process of giving way to an emerging order characterised increasingly by multipolarity. Major power rivalry and geopolitical tension are on the rise. Unilateral action and protectionism are gaining momentum. The United Nations (UN) faces an existential crisis. International law is under enormous assault. All of these pose a direct and serious risk to Africa.
This policy brief presents a brief assessment of the current state of Africa’s engagement with major powers and its readiness for advancing its interests in view of the deep shifts in the global context. Based on such assessment and having regard to the efforts of other parts of the world for repositioning themselves, the brief outlines the kind of major strategic shifts that Africa needs to adopt promptly for repositioning itself for the new international order and to ameliorate the perils the state of the world poses to Africa.
Provisional Programme of Work of the Peace and Security Council for August 2025
Provisional Programme of Work of the Peace and Security Council for August 2025
Date | August 2025
In August, the Republic of Algeria will assume the chairship of the African Union (AU) Peace and Security Council (PSC). The Provisional Programme of Work (PPoW) for the month outlines eight substantive sessions covering nine agenda items and a field mission to South Sudan. All sessions are scheduled to take place at the ambassadorial level. Only two of the nine agenda items will focus on country-specific situations, while the other seven will address thematic issues and PSC’s meetings with relevant bodies.
The first session of the month, scheduled for 4 August, is set to consider the evolving situation in Sudan. This session follows a sequence of high-level engagements by the PSC, the most recent being its 1292nd meeting on 29 July 2025, which came in direct response to the 26 July 2025 announcement by the Rapid Support Forces (RSF) of the establishment of a parallel civilian administration, referred as the Sudan Founding Alliance (Tasis) in areas under its control. The PSC, during this emergency ‘meeting’ held via email exchange, strongly condemned and rejected the formation of this so-called ‘parallel government,’ affirming the AU’s unwavering commitment to the sovereignty, unity, and territorial integrity of Sudan. The Council emphasised that the AU recognises ‘only the Transitional Sovereignty Council and the recently formed civilian transitional government’ until a consensual arrangement is reached that aligns with the aspirations of the Sudanese people. These pronouncements came just months after the Council’s 1261st Summit-level session held on 14 February 2025, on the margins of the 38th AU Summit, which had attracted the participation of high-level figures including AU Commission Chairperson Moussa Faki Mahamat, IGAD Chair Djibouti (represented by its Foreign Minister), UN Secretary-General António Guterres, and a representative from the League of Arab States. Despite the elevated diplomatic engagement at the February summit, the meeting failed to produce substantive decisions. Its outcome communiqué simply reiterated prior calls, such as a humanitarian truce, that both the Sudanese Armed Forces (SAF) and RSF disregarded. Since February, the conflict in Sudan has evolved further. The RSF’s consolidation of control in parts of the west and south, alongside its establishment of a competing political authority, has intensified fears of territorial fragmentation of Sudan along the lines of what is playing out in Libya. Meanwhile, the SAF has maintained its dominance in the north and east, bolstering its presence in strategic areas, while trying to consolidate the diplomatic edge it has over the RSF in regional and international forums.
Despite the persistence of the fragmentation of the diplomatic space and lack of effective diplomatic engagement in recent months, efforts are underway for reinvigorating diplomacy. Egypt has increased bilateral engagements focused on containing instability along the Sudan-Libya-Egypt border, triggered by incidents involving the RSF. On the international front, before its postponement the U.S. was set to convene a peace talk that set to start on 29 July in Washington with Saudi Arabia, the United Arab Emirates, and Egypt to revive the ‘Quad’ initiative, emphasising dialogue over military action. Simultaneously, the U.N. is preparing mediation efforts led by envoy Ramtane Lamamra, coordinating with the AU in Addis Ababa and focusing on talks for civilian protection, aiming to bring the Sudanese parties into proximity negotiations as soon as possible. It is therefore expected that the PSC will discuss these recent developments and follow up on its previous decisions, such as investigations into human rights violations, a plan for civilian protection, and identifying external actors involved in supplying arms and financial support, fueling the fire of the war in Sudan.
On 6 August, the second substantive session will assess the role of ad hoc governance, peace, and security mechanisms in supporting the PSC’s mandate. This will be the first time that PSC will be assessing the effectiveness of ad hoc mechanisms in the implementation of its mandates. The Protocol Relating to the Establishment of the PSC authorises the PSC to establish subsidiary bodies as needed. Specifically, Article 8(5) empowers the PSC to create such bodies, including ad hoc committees, as it deems necessary to undertake tasks such as mediation, conciliation, or fact-finding enquiries. In operational practice, the PSC exercises this mandate through formal communiqués and AU Assembly decisions, which authorise or request the establishment of these mechanisms in the form of ad hoc committees or high-level panels. The session is expected to reflect on how such mechanisms contribute to conflict prevention, mediation, and post-conflict reconstruction. Against the backdrop of increasingly complex crises across the continent, the session provides a timely opportunity to assess the lessons learned from the operation of such mechanisms in reviewing the African Peace and Security Architecture, for making it fit for the evolving and complex security situation and geopolitical context of the continent. The Council is anticipated to examine how these bodies support early warning, strategic mediation, and inclusive dialogue, while also identifying the challenges facing them and ways of adapting them to the fundamentally changing realities of Africa and the world.
On 8 August, the PSC will convene its session dedicated to consultations with the AGA-APSA Platform and the PRC Sub-Committee on Human Rights. During the 1098th session in August 2022, an inaugural consultation was held between the PSC and the AGA-APSA Platform, which decided to institutionalise and regularise this engagement as an annual event. A similar decision was taken at the 1095th session of the PSC, which was held for consultation with the PRC Sub-Committee on Human Rights, Democracy and Governance, affirming that these joint engagements should also be held annually. In August 2023, during its 1167th session, the PSC brought together both mechanisms, the AGA-APSA Platform and the PRC Sub-Committee, for a joint consultation, recognising their shared mandate in promoting governance, democratisation, and constitutionalism. Although these consultations were intended to be held annually, no session took place in 2024. The upcoming consultation is expected to reinvigorate and deepen collaboration among PSC members, the PRC Sub-Committee, and the AGA-APSA Platform. It will build on past engagements, evaluate progress in fulfilling joint commitments, and explore innovative approaches to strengthen coordination in promoting the AU’s shared values.
Between its scheduled sessions, the PSC will conduct a field mission to South Sudan from 10 to 12 August. The visit comes against the backdrop of the escalating political and security crisis that threatens to unravel the hard-won gains of the Revitalised Agreement on the Resolution of the Conflict in South Sudan (R-ARCSS). During its 1283rd session, the PSC voiced deep concern over the deteriorating situation, warning of the risk of a full-scale war due to serious ceasefire violations, the detention of political figures, and a growing erosion of trust among the signatories to the agreement. The field mission will provide the PSC with an opportunity to directly assess the situation on the ground, engage with key stakeholders, including the Revitalised Transitional Government of National Unity (RTGoNU), civil society actors, and regional partners and reinforce its calls for an immediate cessation of hostilities, the unconditional release of political detainees, and the full implementation of the R-ARCSS.
On 13 August, the PSC will convene the only open session of the month to discuss the theme ‘Education in Conflict Situations.’ The last time the Council considered this particular theme was in August 2024 during its 1229th meeting, in which it decided to ‘regularise the Open Session as an annual event of the Council.’ It is expected to build on and follow up on its previous commitments which included, but not limited to, the need for establishing a quality control mechanism to monitor and evaluate inclusive education initiatives to ensure effectiveness and accountability; the need for improving data collection and evidence-based policymaking, to effectively address the unique challenges facing education in conflict situations; and the proposal of mainstreaming inclusive education as an integral component of post-conflict reconstruction and development (PCRD) in countries emerging from conflict situations. The session is also expected to advance its discussions from the recent PSC sessions held in July 2025 on the humanitarian situation in Africa and rehabilitation and reintegration of children formerly associated with armed conflicts, as these naturally extend to education. This meeting also comes just a few months before the AU Education Summit 2025 – a conference aimed at rallying the AU member states, schools and educators from the African continent behind the AU strategic objective that seeks to address the educational challenges the African continent faces.
On 15 August, the PSC will convene to consider two agenda items, beginning with a discussion on the Terms of Reference (ToRs) for the PSC Sub-Committee on Counter-Terrorism. Although the Sub-Committee has long been part of the PSC’s structure, it has never been operationalised since its establishment. During its 1182nd meeting in October 2023, the PSC underscored the importance of fully activating and operationalising the Sub-Committee. In preparation for the Ambassadorial-level session, the Committee of Experts is scheduled to meet tomorrow (1 August) to deliberate on the ToRs.
The second part of the session will be dedicated to the consideration and adoption of the PSC Field Mission Report on South Sudan. Building on the objectives of the field visit and the key findings outlined in the report, the Council is expected to reflect on the current state of the escalating political and security situation. The session will provide an opportunity to assess the impact of recent developments and guide the PSC’s next steps in supporting the implementation of the Revitalised Agreement on the Resolution of the Conflict in South Sudan (R-ARCSS), as well as to address and resolve the ongoing violence in South Sudan.
On 25 August, the PSC will hold its second annual consultative meeting with the Southern African Development Community (SADC) Organ on Politics, Defence and Security. This meeting, scheduled to take place virtually, builds on the commitment made during the inaugural session held on 30 August 2024 in Gaborone, Botswana, where both parties agreed to institutionalise annual consultations alternating between Addis Ababa and Gaborone. Rooted in Article 16 of the PSC Protocol and the 2008 Memorandum of Understanding between the AU Commission and RECs/RMs, the meeting reflects efforts to strengthen coordination and collaboration in promoting peace and security in the region. The consultative session is expected to assess progress made since the inaugural meeting, particularly in light of developments in eastern DRC and in terms of enhancing joint efforts in resource mobilisation for peace operations.
On 27 August, the PSC will convene for a briefing on the early warning system and its role in mapping risks and threats across Africa. The session will feature contributions from key AU institutions, including the African Peer Review Mechanism (APRM), the Committee of Intelligence and Security Services of Africa (CISSA), the AU Mechanism for Police Cooperation (AFRIPOL), and the AU Counterterrorism Centre (AUCTC). This session is expected to provide a comprehensive analysis of political, security, and socio-economic dynamics shaping existing and emerging conflict and security challenges on the continent, building on the AU’s commitment to preventive diplomacy and conflict prevention as outlined in the PSC Protocol and the African Peace and Security Architecture (APSA). The session follows related PSC engagements, including most recently the 1247th session held on 27 November 2024, where CISSA, AUCTC, and AFRIPOL briefed the PSC on the Continental Early Warning and Security Outlook. During that session, the PSC emphasized the need for enhanced collaboration and information sharing among Member States and international partners to counter the exploitation of digital platforms by terrorist and extremist groups and tasked the AUCTC, CISSA, AFRIPOL, and other specialized AU agencies to collaborate with Member States toward establishing a joint Cybersecurity Task Force to prevent the use of information and communication technologies (ICTs) and emerging technologies for radicalization, recruitment, training, and funding by terrorist groups. Furthermore, the 1251st PSC session on 17 December 2024 underscored the need for greater visibility and prominence of CEWS within the proposed restructuring of the Political Affairs, Peace and Security (PAPS) Department, signalling a push for institutional reforms to enhance CEWS’s operational efficiency. Additionally, the 4th Joint Consultative Meeting between the PSC and APRM on 7–8 April 2025 highlighted the importance of leveraging APRM’s governance-focused peer review reports to enhance early warning strategies, building on prior pronouncements which emphasised closer coordination between APRM and PSC to address structural vulnerabilities and governance deficits that fuel conflicts. The upcoming session offers an opportunity to explore how early warning analysis would be holistic by going beyond the recent intelligence and security-focused analysis from CISSA, AFRIPOL, and AUCTC and including APRM’s governance-centred and CEWS all-encompassing analyses. Discussions may also address challenges such as Member States’ denialism of early warning reports, as noted in previous sessions, and the need for enhanced coordination with Regional Economic Communities (RECs) to tackle transnational threats like terrorism, cybercrime, and human trafficking.
The last meeting of the Council will be held on 29 August, which will be a briefing by the African Members to the UN Security Council. Algeria, Sierra Leone and Somalia, serving as non-permanent members for the 2024 – 2025 term are expected to brief the UNSC on several critical peace and security issues on the continent which is expected to include the security situation in eastern DRC, Sudan’s ongoing civil war and humanitarian crisis, South Sudan’s political and security developments, push for UNSC reform and African representation, regional Counter-terrorism in West Africa and the Sahel and cooperation with regional organizations. This meeting comes after the PSC recently adopted the ‘Manual on the Modalities for Enhancing Coordination Between the PSC and the African Members of the United Nations Security Council (A3)’ at its 1289th meeting of 24 July 2025. From the manual, it highlights that, to bolster A3’s influence and impact in the UNSC, the A3 shall consult with relevant stakeholders, including the Non-Aligned Movement and all strategic partners of the AU, on peace and security issues of interest to Africa. In this context, the A3 is tasked with mobilising greater political support in championing the African positions and interests on peace and security issues on the agenda of the UNSC. This being in alignment with the language and commitments from the Conclusions of the 11th Oran Process held in December 2024 in which, it was agreed that there is an imperative to have a synchronization of the meetings of the PSC and those of the UNSC on matters relating to peace, security and stability in Africa, which come under the joint mandate of the two Councils, to ensure proper guidance to the A3 Plus. In addition, it was underscored that there is a need for ensuring a continued push for the A3 to take effective pen-holders or co-pen-holding on African files on the UNSC Agenda. Therefore, the meeting is expected to provide updates on modalities for strengthening coordination between the PSC and A3 based on the experience of the current A3 members and recent trends in the UNSC. The session may also further explore operationalising the manual’s provisions, strategising around UNSC reform efforts, and advancing Africa’s broader multilateral objectives.
